The Whipple
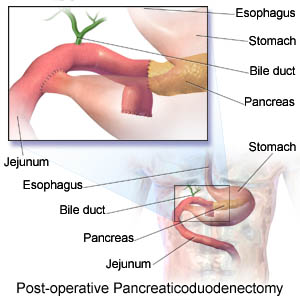
A pancreaticoduodenectomy is often referred to as a Whipple procedure. It is a major surgical operation involving the pancreas, duodenum, and other organs. This operation is performed to treat cancerous tumors on the head of the pancreas, malignant tumors involving common bile duct or duodenum near the pancreas.
A pancreaticoduodenectomy is often referred to as a Whipple procedure. It is a major surgical operation involving the pancreas, duodenum, and other organs. This operation is performed to treat cancerous tumors on the head of the pancreas, malignant tumors involving common bile duct or duodenum near the pancreas.
In the case I assisted in, the patient had already undergone a radical gastrectomy (removal of the stomach). There were several large tumors on the patients pancreas, as well as malignancies on the patients duodenum (the first part of the small intestine). This particular case involved the removal of a major portion of the pancreas and the complete removal of the duodenum, leading to the anastomosis (to join together two hollow organs) of the jejunum (the middle part of the small intestine) to the common bile duct.
I was lucky to be chosen as part of the team, as these cases are so very rare. It was a thrilling experience and I’m glad to have had the opportunity!

A real-life picture, below:
Sorry if this grosses anyone out, but this is what it looked like... and it was SUPER COOL!

This is a pretty good play-by-play of the procedure, but you'll have to picture it without the stomach for the case I was in on. The patient had a long history of cancer.

Patent Ductus Arteriosus
This defect allows blood to mix between the pulmonary artery and the aorta. Before birth an open passageway (the ductus arteriosus) exists between these two blood vessels. Normally this closes within a few hours of birth. When this doesn't happen, some blood that should flow through the aorta and on to nourish the body returns to the lungs. A ductus that doesn't close is quite common in premature infants but rather rare in full-term babies.
If the ductus arteriosus is large, a child may tire quickly, grow slowly, catch pneumonia easily and breathe rapidly. In some children symptoms may not occur until after the first weeks or months of life. If the ductus arteriosus is small, the child seems well. If surgery is needed, the surgeon can close the ductus arteriosus by tying it, without opening the heart. If there's no other defect, this restores the circulation to normal.
Unfortunately for our little patient, the ductus arteriosus was QUITE large and required open heart surgery. The patient was three days old. Tiny, tiny rib spreader. Tiny, tiny suture. But the patient made a full recovery and is now home with mom and dad!
This was my first open-heart surgery. It was incredible. Really intensive. The procedure required a full cardiopulmonary bypass and the heart was stopped for a full 20 minutes!




Tiny! Don't worry, the patient is doing great, and is back at home by now.
No comments:
Post a Comment